< 建議閱讀時間 : 5分鐘>
在香港牙醫體系入面,分為普通科醫生和專科醫生。而專科醫生有八個學科,其中一個學科便是(口腔頜面外科)。而我們所講的轉介到專科醫生剝牙就是指他們。
為甚麼要轉介到專科醫生那裏呢
主要分為兩大類別:
第一 : 難度
影響難度因素有幾個:
1. 病歷:
如果病人本身患有一些疾病 ( 嚴重糖尿病) 或者正在進行藥物治療 ( 例如服食薄 血藥), 就會考慮是否需要轉介到專科醫生。
2. 年齡:
一般來說,年紀愈大,牙骨愈硬,愈難脫牙。而分水嶺就是35歲。這亦是為什麼 American Association of Oral and Maxillofacial Surgeons 提倡在35歲前決定。
3. 張開口程度:
如果病人張口程度少過 40mm (大約四隻手指闊度),會令到手術視野和範圍減低。

4. 牙齒本身:
先問一個問題
在下列四個種類中,你認為難度最高是那種,最低又是哪種?

.....
.....
.....
.....
難度由淺入深 : Mesioangular < Horizontal < Vertical < Distoangular
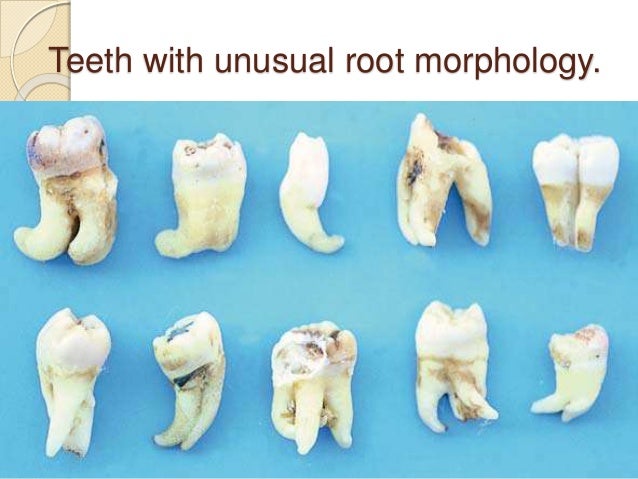
如果牙齒本身例如牙腳彎曲,叉開等等,都會大大增加手術的難度。如圖下:
另外,比較少發生的是智慧齒附近牙肉組織出現病變,如下圖。這個時候就一定需要轉介去診斷和治療了。

左下智慧齒出現了dentigerous cyst (齒源性囊腫)
第二 : 風險
在脫下智慧齒時,特別要提及有可能兩條神經線受傷的風險: 舌神經和下齒槽神經。
在眾多文獻中,得中的結論是兩條神經線受傷的風險都很低(少過3-4%)。
其中一個令到風險降低原因正正是醫生適當地將複雜又高近神經線的智慧齒轉介到專科醫生
那裏。
接不來你又會問,去到專科醫生那裏又會做甚麼?
第一,醫生會分析個案,再決定是否需要CT scan,也就是我們說的電腦掃瞄。
第二,醫生會決定手術模式,如果他認為難度較高較複雜,便需要全身麻醉。如做全身麻
醉,通常會在同一個手術把所有阻生智慧齒也脫除。
如果醫生認為牙腳很接近神經,就會選擇牙冠切除法 -- 會把部份沒感染的牙腳留在牙
骨槽,牙肉和牙骨會把牙冠埋沒,令神經線受損機會非常低。只有非常少數情況牙腳若干年
露出口腔,到時便需要把它取走,不過那時候傷及神經的風險非常低,因為牙腳已離開了神
經一段距離。

牙冠切除法 手術前後
總括而論,不是所有個案普通科醫生也可以處理,但亦不是所有個案也需要專科醫生脫
。請相信您的醫生的專業判斷,如有疑惑,亦可以提出,因為醫生希望看見是,希望病人在
做手術前能夠明白理解當中手術步驟、風險等,作有效溝通。最不希望看見的是當手術後真
的出了後遺症,而病人後悔埋怨等等情況發生。
********************************************************************************
<Recommended reading time: 5 minutes>
The Hong Kong dental system is divided into general practitioners and specialists. Specialists have eight disciplines, one of which is (oral and maxillofacial surgery). And when we talk about referrals to specialists for removal of teeth, it's referred to them.
Why are you referred to a specialist?
There are two main categories:
First: Difficulty
There are several factors that affect difficulty:
1. Medical record
If the patient has some illness (severe diabetes) or is undergoing medication (such as taking anticoagulent drug ) he will consider whether a referral to a specialist is needed.
2. Age:
Generally speaking, the older you are, the harder your bone are and the harder it is to get rid of them. The critical age is 35 years old. That's why the American Association of Oral and Maxillofacial Surgeons advocates making decisions before the age of 35.
3. Mouth opening degree:
If the patient's mouth opening is less than 40mm (approximately four digits s wide), the surgical field of vision and range will be greatly reduced.
4. The teeth themselves:
Ask a question first
OUT of the following four categories, which one do you think is the most difficult and which is the lowest?
Answer:
Difficulty from shallow to deep: Mesioangular <Horizontal <Vertical <Distoangular
If the roots of teeth themselves are bent, they will greatly increase the difficulty of surgery. As shown below:
In addition, it is relatively rare for lesions in the dental tissues near the wisdom teeth to occur, as shown below. However, it does happen. At this time, you must be referred for diagnosis and treatment.
Dentigerous cysts appear in the lower left wisdom tooth
Second: Risk
When removing wisdom teeth, mention in particular the risk of injury to two nerves: the lingual nerve and the inferior alveolar nerve.
In many literatures, it has been concluded that the risk of injury to both nerve wires is low (less than 3-4%).
One of the reasons that reduces the risk is appropriate referral of complex and high-end nerve to a specialist
If you can't get it, you will ask again, what will you do when you go to the specialist?
First, the doctor will analyze the case and decide whether a CT scan is needed, which is what we call a computer scan.
Second, the doctor decides the mode of surgery. If he thinks the difficulty is more complicated, he needs general anesthesia. General anesthesia is like put u into sleep, usually required when removing all impacted wisdom teeth in the same operation or in some difficult cases.
If the doctor thinks that the roots are close to the nerves, he will choose the crown resection method and leave some uninfected roots in the teeth bury under bone. The chance of damaging the nerve wire is very low. Very few cases the root becomes exposed into the mouth and it needs to be removed at that time, but the risk of injury to the nerves at that time is very low, because the roots has migrated away from the nerve.
After some distance.
Crown resection before and after surgery
In a nutshell, not all cases can be handled by general practitioners, but not all cases also require specialists
. Please trust your doctor's professional judgment. If you have any doubts, you can also raise it, because the doctor wants to patient take part in the decision making and understand the surgical procedures, risks, etc., and communicate effectively before surgery. The last thing we want to see is patient without the consent and unfortunate things happen.
Source:
1. https://www.aaoms.org/docs/govt_affairs/advocacy_white_papers/management_third_molar_white_paper.pdf)
留言
發佈留言